
Your support changes lives. Thank you!
Learn More
Discover a structured framework for assessing patients’ AI chatbot use, including its frequency,…


In the practice of Cognitive Behavioral Therapy (CBT), upsetting moods and negative behaviors are overcome using our thoughts and logic. CBT therapists help clients identify irrational, upsetting core beliefs, and then use rational counter thoughts to defeat those beliefs. This strategy has been shown in research to be quite effective; and the reason is obvious - feelings change, but facts don't. A solid fact is preferable to shaky emotional ground any day.
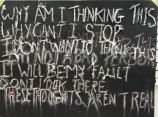
Yet, in the treatment of OCD, the strategy can backfire. OCD is brutal. Obsessions seek to make you rethink everything; doubting your beliefs, perceptions, or emotions (as in Relationship OCD), your actions (Safety and Contamination OCD), and even your morals and self-identity (Harm OCD, Homosexuality OCD). So, MORE thinking, even seemingly rational thinking, does not equate to LESS ruminating. We find that, typically, it's unhelpful to try to reason with your intrusive thoughts.
However, CBT has been found to be, in general, the most effective psychotherapy for anxieties. So, what to do? It's not a matter of a different therapeutic modality, but rather a different strategy. One of the strategies is this: We do not hang out with bullies.
You remember the bully from school. They call your name, demean you, undermine your confidence. Bullies notice where their victim’s weaknesses lie, and attack where they’re vulnerable. There’s the verbal harassment, the continual taunting. And the threats – there’s always an implication, overt or covert, that if you don’t comply, things will get worse.
But as we all know, giving in to a bully does not engender kindness in return, but rather, more bullying. When the victim acquiesces, the bully may back down for a moment, only to return the next day with more taunts, more demands.
The same is true for the “bully” that is your OCD thoughts. These thoughts are not helpful things to consider in order to improve your life. This bully will only serve to make you fearful, intimidated, and immobilized. OCD holds out a promise of freedom and peace; while in reality, compulsions deliver only momentary relief followed by more obsessive thoughts, and increasingly intense compulsive urges. In therapy, our strategy shifts from examining thought content details to determining the pattern these thoughts take, and to learn to recognize that pattern for the bully it is.
For example, a common anxious thought might be fear of failing an exam. In non-OCD patients, psychologists might help the patient remind herself of the amount of preparation she did, her history of being a successful student, or the fact that one grade does not make or break a semester. These cognitive interventions refocus the mind on the facts, or the “most likely” scenario, as opposed to the worst-case scenario.
But in OCD, the strategy is completely different. An OCD patient faces an exam, and that’s where the mental bullying begins:
“You better wear your lucky sweater – and where is it, by the way?” the bully might ask.
“Have you really studied enough?”
“better check with your professor about that question again”
And so on.
So the OCD bully’s victim feels compelled to engage in superstitions. Or she may engage in repeated checking behaviors, such as asking the professor and her classmates unending clarifying questions. These may provide momentary reassurance, while long-term setting the student up for increased anxiety, and decreased confidence in her own abilities.
Therapeutically, the goal is NOT to reason with the fear. The goal is to help the patient see that these thoughts follow the same M.O. as previous OCD-driven thoughts, and to refuse to entertain the OCD-driven demands.
Just as you would not endeavor to build your life around what a 7th grade bully said about you, you don't build your life around the mental and behavioral hoops OCD is trying to make you jump through. You learn to listen past the content of the thoughts, recognizing the pattern and realizing you don't need to engage. (Remember how engaging the 7th grade bully just emboldened them?) Instead, you see the bully coming and shut the door. There’s no reason to hear what he has to say.
This takes practice and work in therapy, of course. But this strategy prevents OCD sufferers from expending effort on futile missions. Once this strategy is adopted, we can proceed to other parts of the treatment, such as Exposure and Response Prevention (ERP).
OCD treatment is not easy; but, in some ways it is simple:
This post is presented in collaboration with ADAA's OCD and Related Disorders SIG. Learn more about the SIG.

Take Action
Find Help. Learn More. Support ADAA.












ADAA Blog Content and Blog Comments Policy
ADAA provides this Website blogs for the benefit of its members and the public. The content, view and opinions published in Blogs written by our personnel or contributors – or from links or posts on the Website from other sources - belong solely to their respective authors and do not necessarily reflect the views of ADAA, its members, management or employees. Any comments or opinions expressed are those of their respective contributors only. Please remember that the open and real-time nature of the comments posted to these venues makes it is impossible for ADAA to confirm the validity of any content posted, and though we reserve the right to review and edit or delete any such comment, we do not guarantee that we will monitor or review it. As such, we are not responsible for any messages posted or the consequences of following any advice offered within such posts. If you find any posts in these posts/comments to be offensive, inaccurate or objectionable, please contact us via email at [email protected] and reference the relevant content. If we determine that removal of a post or posts is necessary, we will make reasonable efforts to do so in a timely manner.
ADAA expressly disclaims responsibility for and liabilities resulting from, any information or communications from and between users of ADAA’s blog post commenting features. Users acknowledge and agree that they may be individually liable for anything they communicate using ADAA’s blogs, including but not limited to defamatory, discriminatory, false or unauthorized information. Users are cautioned that they are responsible for complying with the requirements of applicable copyright and trademark laws and regulations. By submitting a response, comment or content, you agree that such submission is non-confidential for all purposes. Any submission to this Website will be deemed and remain the property of ADAA.
The ADAA blogs are forums for individuals to share their opinions, experiences and thoughts related to mental illness. ADAA wants to ensure the integrity of this service and therefore, use of this service is limited to participants who agree to adhere to the following guidelines:
1. Refrain from transmitting any message, information, data, or text that is unlawful, threatening, abusive, harassing, defamatory, vulgar, obscene, that may be invasive of another 's privacy, hateful, or bashing communications - especially those aimed at gender, race, color, sexual orientation, national origin, religious views or disability.
Please note that there is a review process whereby all comments posted to blog posts and webinars are reviewed by ADAA staff to determine appropriateness before comments are posted. ADAA reserves the right to remove or edit a post containing offensive material as defined by ADAA.
ADAA reserves the right to remove or edit posts that contain explicit, obscene, offensive, or vulgar language. Similarly, posts that contain any graphic files will be removed immediately upon notice.
2. Refrain from posting or transmitting any unsolicited, promotional materials, "junk mail," "spam," "chain mail," "pyramid schemes" or any other form of solicitation. ADAA reserves the right to delete these posts immediately upon notice.
3. ADAA invites and encourages a healthy exchange of opinions. If you disagree with a participant 's post or opinion and wish to challenge it, do so with respect. The real objective of the ADAA blog post commenting function is to promote discussion and understanding, not to convince others that your opinion is "right." Name calling, insults, and personal attacks are not appropriate and will not be tolerated. ADAA will remove these posts immediately upon notice.
4. ADAA promotes privacy and encourages participants to keep personal information such as address and telephone number from being posted. Similarly, do not ask for personal information from other participants. Any comments that ask for telephone, address, e-mail, surveys and research studies will not be approved for posting.
5. Participants should be aware that the opinions, beliefs and statements on blog posts do not necessarily represent the opinions and beliefs of ADAA. Participants also agree that ADAA is not to be held liable for any loss or injury caused, in whole or in part, by sponsorship of blog post commenting. Participants also agree that ADAA reserves the right to report any suspicions of harm to self or others as evidenced by participant posts.