Your support changes lives. Thank you!
Learn More
Discover a structured framework for assessing patients’ AI chatbot use, including its frequency,…


Obsessive-Compulsive Disorder is a complicated and debilitating mental illness. By the definition in the Diagnostic Statistical Manual (APA, 2013), OCD is classified as a neurological disorder where a person will perform a series of rituals or compulsions in response to persistent and unwanted intrusive thoughts or obsessions. Many experts and researchers consider OCD to be a syndrome because it includes other disorders, such as depression, anxiety disorders, panic disorder, eating disorders, and so on. Some of the most common co-occurring disorders are trichotillomania (hair-pulling), dermatillomania (skin-picking), and Body Dysmorphic Disorder (BDD). All of these disorders occur alongside OCD so often, they are considered part of the spectrum of obsessive-compulsive behaviors, not unlike the autistic spectrum. In order to better understand these disorders and their relationship to OCD, we must first understand the difference between compulsive behavior and impulsive behavior.
In evaluating these disorders, it is key to identify whether a person’s actions are impulsive or compulsive. If a behavior is compulsive, it is seen as something unpleasant and distressing. For example, a patient can understand that flipping a light switch on and off in multiples of three will not prevent bad things from happening to them, but they feel they have no choice to not perform this task. Conversely, impulsive behavior, such as shoplifting or binge drinking, is more consistent with satisfying an urge that is pleasurable rather than disturbing and may not understand the consequences of their actions. These actions can also be described on a spectrum, as illustrated in the image below.
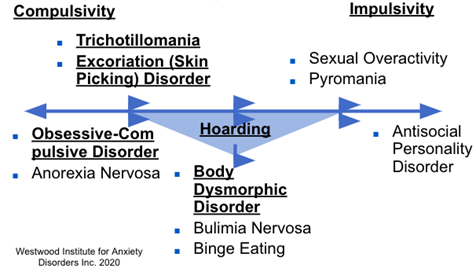
Compared to disorders such as pyromania and Antisocial Personality Disorder (ASPD), OCD, BDD, trichotillomania, and dermatillomania are known as compulsive disorders rather than impulsive. They are not reflective of a person’s core values or personality and are due to an underlying neurological condition. On the other hand, an individual with ASPD will find the impulsive behavior pleasurable instead of disturbing, thereby making it more likely that they will lean into the behavior.
Body Dysmorphic Disorder is defined by an excessive preoccupation with one’s own appearance. This disorder falls under compulsive disorders on the spectrum and can be treated with medication and Cognitive Behavioral Therapy specializing in exposure sessions for the patient. One of the unique exposure techniques used at the Westwood Institute is the “crooked mirror” exposure, which involves a patient observing a purposely distorted image of their body in order to acclimate them to the anxiety they feel about their body. What distinguishes BDD from OCD is the person’s focus on the body and the delusion that there is something wrong with their appearance. The delusional aspect of these beliefs puts BDD somewhere in the middle of the spectrum between compulsivity and impulsivity because the patient believes that their body is incorrect due to perceived flaws and imperfections which is not objectively true. When evaluating a patient, it is paramount that the clinician make the distinction between these disorders, as it will make the difference between recovery and worsening of symptoms.
Trichotillomania, or hair-pulling, is classified under Body-Focused Repetitive Behaviors (BFRB) and considered a compulsive disorder. However, it is noted in certain cases that a person may find hair-pulling to be a pleasurable activity, making it more of an impulsive behavior than compulsive. Because of this, the better choice of treatment may be abstinence combined with other forms of cognitive behavioral therapy such as exposure sessions that ask the patient to sit without pulling out any hairs or wear rubber finger covers until the therapist feels they will not pull on their hair. This is similar to breaking the habit of biting your nails or sucking your thumb. Like OCD, trichotillomania can also be managed with medications such as SSRIs and has shown to be most effective when combined with therapy.
Dermotillomania, or skin-picking, is also considered a BFRB and falls on the compulsive end of the spectrum. Skin-picking is particularly destructive to an individual’s physical appearance, as the habit can cause bleeding, bruising, infections, or permanent disfigurement. This disorder is also treated with medication, HRT, and ExRP, but the success treatment will depend on how well they understand their own issues. Higher levels of insight are more associated with compulsive behavior because it causes the person to feel more anxious due to their perceived lack of control. On the other hand, lower levels of insight are more associated with impulsive behaviors because the person may not understand what effect their actions have on themselves and others. This is also why the proper assessment of these behaviors cannot be stressed enough. Patients and clinicians alike must work together in order for the treatment to be successful.
For more information on research concerning OCD and related disorders, please contact the Westwood Institute for Anxiety Disorders in Los Angeles, CA at our website: www.hope4ocd.com or email us at [email protected]. Additional information about OCD can be found on the ADAA website.
Special thanks to Rebecca Braverman for her assistance in writing this blog.

Take Action
Find Help. Learn More. Support ADAA.












ADAA Blog Content and Blog Comments Policy
ADAA provides this Website blogs for the benefit of its members and the public. The content, view and opinions published in Blogs written by our personnel or contributors – or from links or posts on the Website from other sources - belong solely to their respective authors and do not necessarily reflect the views of ADAA, its members, management or employees. Any comments or opinions expressed are those of their respective contributors only. Please remember that the open and real-time nature of the comments posted to these venues makes it is impossible for ADAA to confirm the validity of any content posted, and though we reserve the right to review and edit or delete any such comment, we do not guarantee that we will monitor or review it. As such, we are not responsible for any messages posted or the consequences of following any advice offered within such posts. If you find any posts in these posts/comments to be offensive, inaccurate or objectionable, please contact us via email at [email protected] and reference the relevant content. If we determine that removal of a post or posts is necessary, we will make reasonable efforts to do so in a timely manner.
ADAA expressly disclaims responsibility for and liabilities resulting from, any information or communications from and between users of ADAA’s blog post commenting features. Users acknowledge and agree that they may be individually liable for anything they communicate using ADAA’s blogs, including but not limited to defamatory, discriminatory, false or unauthorized information. Users are cautioned that they are responsible for complying with the requirements of applicable copyright and trademark laws and regulations. By submitting a response, comment or content, you agree that such submission is non-confidential for all purposes. Any submission to this Website will be deemed and remain the property of ADAA.
The ADAA blogs are forums for individuals to share their opinions, experiences and thoughts related to mental illness. ADAA wants to ensure the integrity of this service and therefore, use of this service is limited to participants who agree to adhere to the following guidelines:
1. Refrain from transmitting any message, information, data, or text that is unlawful, threatening, abusive, harassing, defamatory, vulgar, obscene, that may be invasive of another 's privacy, hateful, or bashing communications - especially those aimed at gender, race, color, sexual orientation, national origin, religious views or disability.
Please note that there is a review process whereby all comments posted to blog posts and webinars are reviewed by ADAA staff to determine appropriateness before comments are posted. ADAA reserves the right to remove or edit a post containing offensive material as defined by ADAA.
ADAA reserves the right to remove or edit posts that contain explicit, obscene, offensive, or vulgar language. Similarly, posts that contain any graphic files will be removed immediately upon notice.
2. Refrain from posting or transmitting any unsolicited, promotional materials, "junk mail," "spam," "chain mail," "pyramid schemes" or any other form of solicitation. ADAA reserves the right to delete these posts immediately upon notice.
3. ADAA invites and encourages a healthy exchange of opinions. If you disagree with a participant 's post or opinion and wish to challenge it, do so with respect. The real objective of the ADAA blog post commenting function is to promote discussion and understanding, not to convince others that your opinion is "right." Name calling, insults, and personal attacks are not appropriate and will not be tolerated. ADAA will remove these posts immediately upon notice.
4. ADAA promotes privacy and encourages participants to keep personal information such as address and telephone number from being posted. Similarly, do not ask for personal information from other participants. Any comments that ask for telephone, address, e-mail, surveys and research studies will not be approved for posting.
5. Participants should be aware that the opinions, beliefs and statements on blog posts do not necessarily represent the opinions and beliefs of ADAA. Participants also agree that ADAA is not to be held liable for any loss or injury caused, in whole or in part, by sponsorship of blog post commenting. Participants also agree that ADAA reserves the right to report any suspicions of harm to self or others as evidenced by participant posts.