
Your support changes lives. Thank you!
Learn More
Discover a structured framework for assessing patients’ AI chatbot use, including its frequency,…


As a clinician specializing in treating clients with anxiety and obsessive-compulsive disorder (OCD), my work involves a lot of thinking. My job also requires me to think about what my clients are obsessively thinking about and how I can help them with the hyperawareness of their thoughts. Thinking, and even overthinking, is normal but when it becomes a mental health disorder, known as hyperawareness OCD, the person feels completely distracted and out of control.
Imagine you have just returned from your daily run and are drinking some water, wiping the sweat from your eyes, blinking to let the moisture settle. Things that would be normal after a run. You turn on the television and are quickly engrossed; however, for just an instant, you are preoccupied by an innocuous thought – the blinking of your eyes. This would usually retreat into the abyss of the mind where most thoughts meet their demise, but in the case of hyperawareness OCD, it remains. Moments turn into minutes, possibly hours, and anxiety erupts into panic.
What is Hyperawareness OCD?
Hyperawareness OCD involves exaggerated and unwanted concerns about normal bodily sensations, functions, or processes that would usually be unconscious. The main fear is that the thought will be permanently embedded in the consciousness, resulting in severe stress and anxiety. One’s internal thinking, their thinking that they shouldn’t be thinking what they are thinking (basically thinking about thinking), and then obsessing about the thinking all become so overwhelming and uncontrollable.
Compared to other OCD themes such as violence, contamination, sex or health, thoughts in hyperawareness OCD seem more “tame” but they can be just as debilitating. Those who suffer from this type of OCD also feel “stuck” but differ in recognizing that there is no real purpose behind the obsession.
While these obsessions seem harmless, troubling and frightening concerns do exist, such as:
Treatment of Hyperawareness OCD
Treatment for this subtype of OCD includes combined approaches of Cognitive Behavioral Therapy (CBT), Exposure and Response Prevention (ERP), and Acceptance and Commitment Therapy (ACT).
In hyperawareness OCD, the person suffering is trying to safeguard the present moment while being over concerned with ruining it. For example, because I am thinking about my blinking, I ought to be thinking about something more satisfying and productive.
CBT is used to challenge how the client interprets these thoughts and gives them a more reasonable and balanced understanding, thereby weakening the OCD story. This works to build confidence so that the client can use both ERP and ACT.
As hyperawareness OCD differs from most OCD, treatment also differs somewhat. Most obsessive compulsive disorders are treated through exposure to the obsession, purposely increasing anxiety while not doing the compulsions, with the idea that over time, the anxiety will decrease. With hyperawareness OCD, the focus of treatment is not so much on the exposure (though some exposures can be helpful) but on response prevention. The goal is to reduce the person’s reaction to bodily sensations by not giving them attention.
When addressing awareness and attention, these terms are often used interchangeably which leads to confusion and inconsistencies with treatment. It is impossible to keep a thought out of awareness, but, if we learn to not give the thought attention, it will go away. In other words, if there is something you want out of your scope of awareness, you cannot force it to leave. The idea is to not actively keep it in your awareness, but to let it go and do nothing. Understanding this difference can be challenging, yet, with practice, we can learn to be aware, allow sensations to exist, and respond without compulsions.
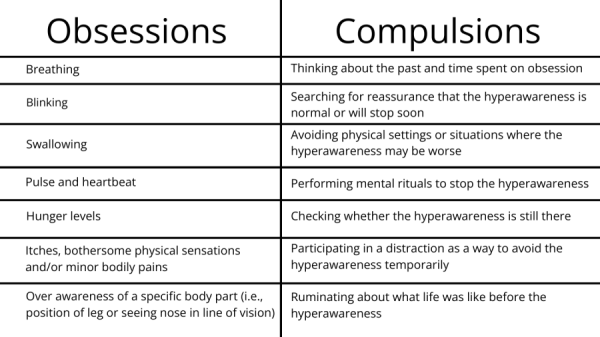
Obsessions and Compulsions in Hyperawareness OCD
While not a complete list, the table below provides some examples of obsessions and compulsions that someone with this type of OCD might experience (note that the examples in each column don’t necessarily correlate):
As a clinician in recovery from hyperawareness OCD, my hope is to educate others on some of the differences of the disorder and what to consider in treatment. Had it not been for the courage and experience of my therapist to educate himself, I most likely would still be “stuck” in “blinking hell.” Instead, I now just accept the fact that “I’m just a guy that thinks about his blinking” and, on most days, my life is brighter.
This post is presented in collaboration with ADAA's OCD and Related Disorders SIG. Learn more about the SIG.


Take Action
Find Help. Learn More. Support ADAA.












ADAA Blog Content and Blog Comments Policy
ADAA provides this Website blogs for the benefit of its members and the public. The content, view and opinions published in Blogs written by our personnel or contributors – or from links or posts on the Website from other sources - belong solely to their respective authors and do not necessarily reflect the views of ADAA, its members, management or employees. Any comments or opinions expressed are those of their respective contributors only. Please remember that the open and real-time nature of the comments posted to these venues makes it is impossible for ADAA to confirm the validity of any content posted, and though we reserve the right to review and edit or delete any such comment, we do not guarantee that we will monitor or review it. As such, we are not responsible for any messages posted or the consequences of following any advice offered within such posts. If you find any posts in these posts/comments to be offensive, inaccurate or objectionable, please contact us via email at [email protected] and reference the relevant content. If we determine that removal of a post or posts is necessary, we will make reasonable efforts to do so in a timely manner.
ADAA expressly disclaims responsibility for and liabilities resulting from, any information or communications from and between users of ADAA’s blog post commenting features. Users acknowledge and agree that they may be individually liable for anything they communicate using ADAA’s blogs, including but not limited to defamatory, discriminatory, false or unauthorized information. Users are cautioned that they are responsible for complying with the requirements of applicable copyright and trademark laws and regulations. By submitting a response, comment or content, you agree that such submission is non-confidential for all purposes. Any submission to this Website will be deemed and remain the property of ADAA.
The ADAA blogs are forums for individuals to share their opinions, experiences and thoughts related to mental illness. ADAA wants to ensure the integrity of this service and therefore, use of this service is limited to participants who agree to adhere to the following guidelines:
1. Refrain from transmitting any message, information, data, or text that is unlawful, threatening, abusive, harassing, defamatory, vulgar, obscene, that may be invasive of another 's privacy, hateful, or bashing communications - especially those aimed at gender, race, color, sexual orientation, national origin, religious views or disability.
Please note that there is a review process whereby all comments posted to blog posts and webinars are reviewed by ADAA staff to determine appropriateness before comments are posted. ADAA reserves the right to remove or edit a post containing offensive material as defined by ADAA.
ADAA reserves the right to remove or edit posts that contain explicit, obscene, offensive, or vulgar language. Similarly, posts that contain any graphic files will be removed immediately upon notice.
2. Refrain from posting or transmitting any unsolicited, promotional materials, "junk mail," "spam," "chain mail," "pyramid schemes" or any other form of solicitation. ADAA reserves the right to delete these posts immediately upon notice.
3. ADAA invites and encourages a healthy exchange of opinions. If you disagree with a participant 's post or opinion and wish to challenge it, do so with respect. The real objective of the ADAA blog post commenting function is to promote discussion and understanding, not to convince others that your opinion is "right." Name calling, insults, and personal attacks are not appropriate and will not be tolerated. ADAA will remove these posts immediately upon notice.
4. ADAA promotes privacy and encourages participants to keep personal information such as address and telephone number from being posted. Similarly, do not ask for personal information from other participants. Any comments that ask for telephone, address, e-mail, surveys and research studies will not be approved for posting.
5. Participants should be aware that the opinions, beliefs and statements on blog posts do not necessarily represent the opinions and beliefs of ADAA. Participants also agree that ADAA is not to be held liable for any loss or injury caused, in whole or in part, by sponsorship of blog post commenting. Participants also agree that ADAA reserves the right to report any suspicions of harm to self or others as evidenced by participant posts.